
2025 marks the 25th anniversary of TB Alliance. Throughout the year, we are sitting down with leaders and visionaries in the TB space in our “Past, Present, and Future of TB Drug Development” series. Ahead of World TB Day, we connected with Dr. Mel Spigelman, President and CEO of TB Alliance. Dr. Spigelman is one of the world’s foremost experts in TB and TB drug development, and the architect of many key TB Alliance innovations, including the regimen-based development paradigm. We discussed the current state of TB Alliance, how the world initially underestimated what would be required to revive TB R&D, the changing landscape of financial and political support for TB research, and the next generation innovations soon to come from TB Alliance and its partners. Read more from our discussion below.
You have been a part of TB Alliance for the vast majority of its history; how have you seen the organization—and the drug development space more broadly—evolve over that time?
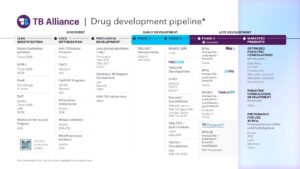
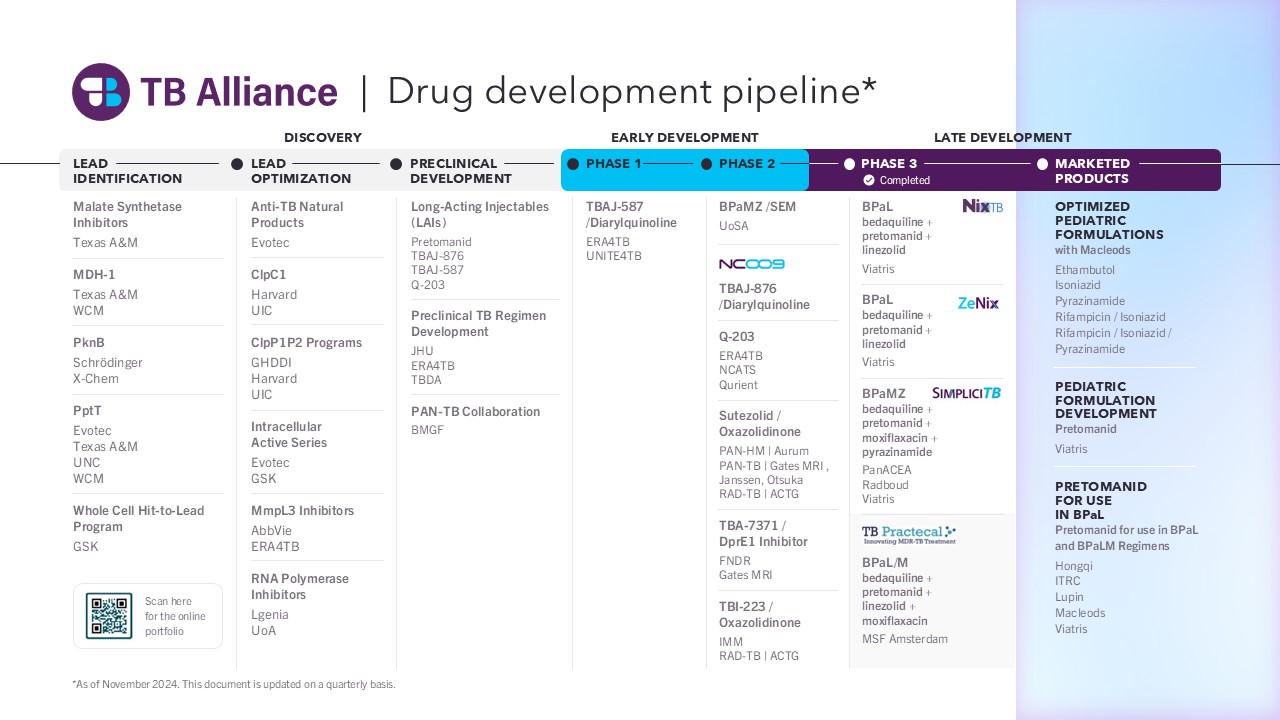
First and foremost, I think we are in an incredible position now, from a scientific perspective. We have the strongest pipeline we have ever had, which includes potential universal regimens for active TB in late-stage development and compounds that could be extremely effective in preventative TB therapy. While our major focus continues to be TB, we now also have a number of exciting and emerging areas of research, like new treatments for adjacent diseases such as leprosy, Buruli ulcer, mycobacterium abscessus and avium. We also are exploring the application of technologies such as long acting injectables as well as immunotherapeutic approaches and artificial intelligence (AI) in markedly enhancing the potential patient benefits from our pipeline.
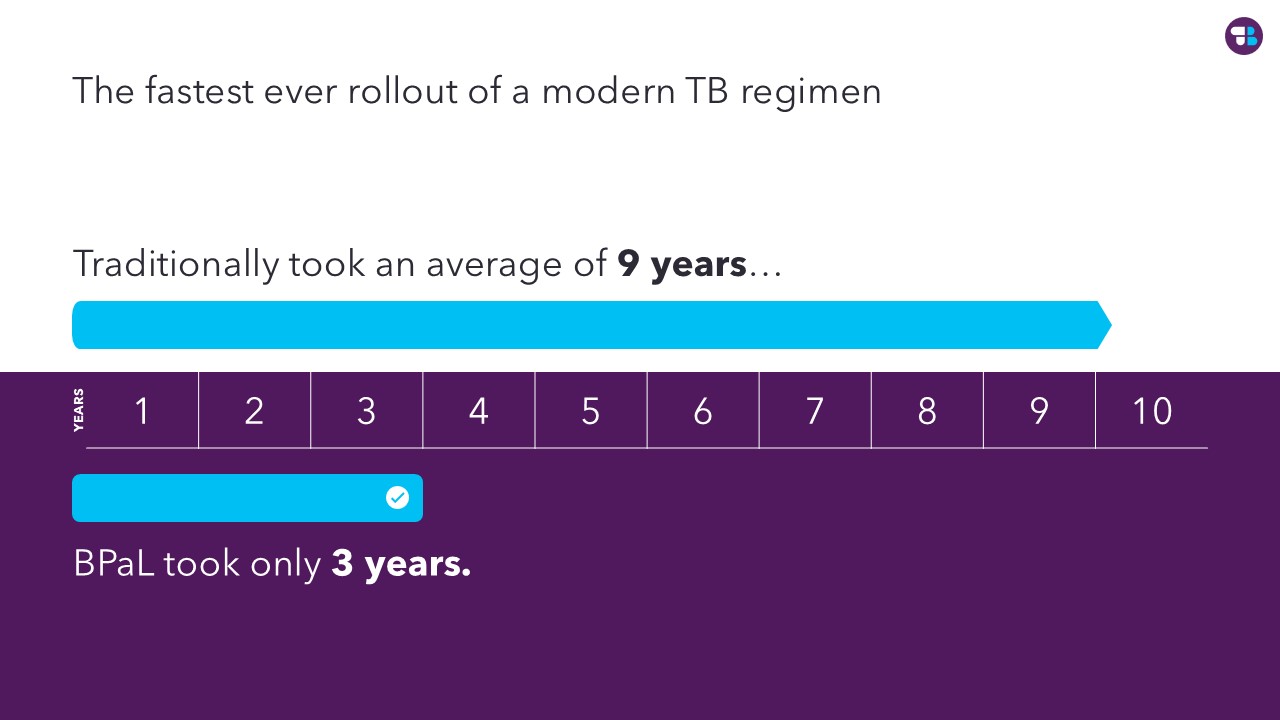
Building off the successes in our R&D work, we also have quickly developed one of the most robust and effective access programs in the global health space – we are really telescoping the time it takes for new treatments to reach all who need them.
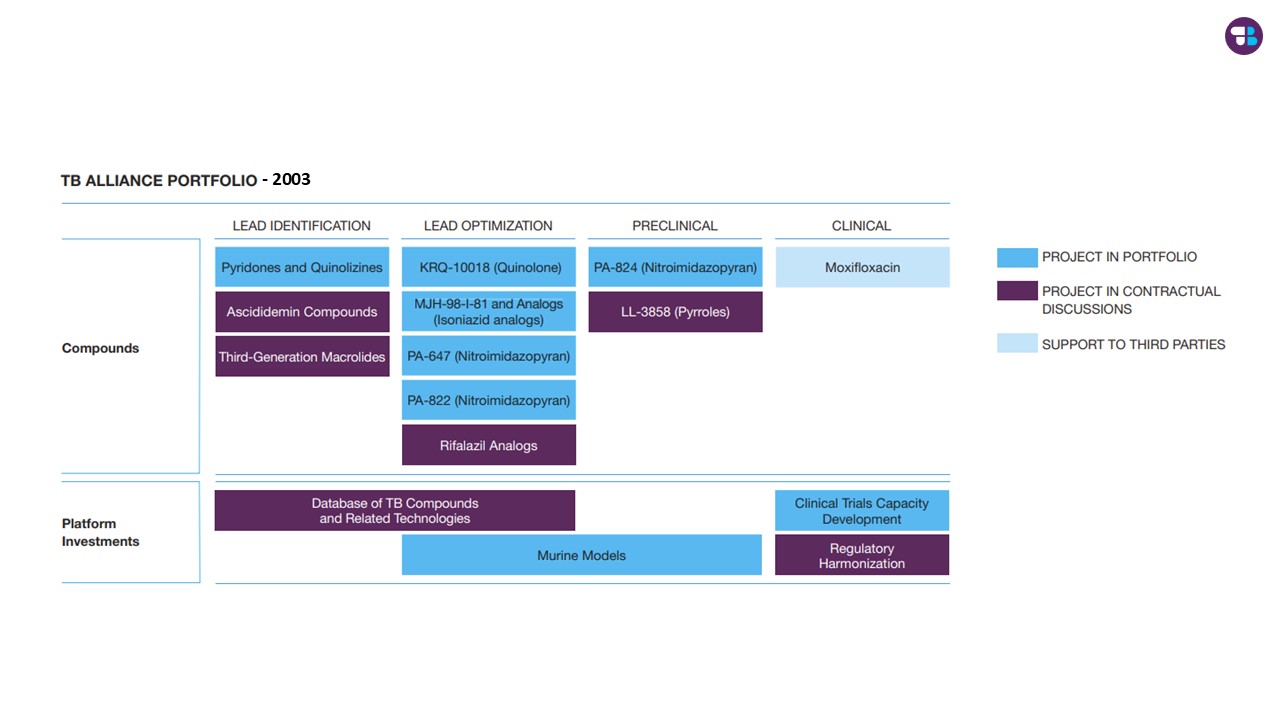
Getting to this place, however, has involved a tremendous amount of learning and adapting. I think in the very early days, TB Alliance was a bit naïve to what would be required to really deliver on the commitment to revolutionize the field of TB therapeutics and get new products to the people who need them.
There was a presumption that there were a lot of promising candidates just sitting on the shelves at pharma companies and somewhat naïve ideas about the allure of the TB market to the for-profit sector, and how uninvolved TB Alliance could be in products access. These assumptions unfortunately proved not to be the case, and consequently, there was significantly more work for the Alliance than originally anticipated.
So, it became clearer and clearer that hurdles to be overcome in delivering on our mission were more formidable than expected when this experiment was conceived. We needed to mobilize, adapt, and expand to overcome them. We had no choice but to grow and become an engine of innovation in drug discovery, trial design, community engagement, access, and more. We built a tremendous network of global partners and expert staff, and have taken advantage of our flexible model to address whatever challenges this mission has thrown at us.
What about global support and funding for the TB research; how has that evolved?
One of the sad ironies is that in our early years, we did not yet have all the ingredients to achieve our mission—a robust pipeline, streamlined development pathways, a refined market access approach, and so on. But we enjoyed a significant amount of political and financial support, as product development partnerships (PDPs) were exciting new entities and thus there was a lot of energy behind organizations like ours.
In the years since its founding, TB Alliance matured substantially, conceiving a new paradigm of TB regimen development, developing a robust pipeline, introducing new treatments for pediatric TB and most recently transforming treatment for drug-resistant TB. Over the last ten-plus years, PDPs have proven to be incredibly productive and cost-efficient developers of new global health technologies. Yet, funding for PDPs like TB Alliance has waned as our scientific output has increased, and as we get closer and closer to achieving our missions and having our biggest impacts yet.
Now, the prospects of further retrenchment of TB R&D come at the exact time increased investment is most critically needed—and would have their highest ROI.

Graphic courtesy of Impact Global Health, from the 2024 G-FINDER Report, which tracks funding for global health R&D
And, how close are you to achieving that mission?
We are closer than ever. I believe we are at a point where we can realistically see a path to ending TB. From a treatment perspective, to make that possible we need a very short and highly effective universal treatment for active TB – a single regimen that could treat virtually all people with TB regardless of their drug resistance profile. We also need an ultra-short treatment for latent TB to address the reservoir of future potential cases. I truly believe we can get there from the drug candidates and regimens currently in our pipeline along with the innovative technologies also currently under investigation. These potential breakthroughs, coupled with the tremendous progress being made in the areas of TB vaccines and diagnostics, make a path to TB eradication very plausible in the not too distant future.



For example, we are currently evaluating the initial results of a pan-Phase 2 trial testing what is potentially the first universal regimen – a combination of TBAJ-876, pretomanid, and linezolid. This regimen, coupled with progress being made with long acting injectables could result in a one-to-two-month regimen for active TB. That would be a tremendous advance for people with TB and for health systems, as it could dramatically shorten and simplify TB treatment, reduce the need for advanced diagnostics, and set the stage for additional cost reductions.
But I think we can do even more than that. What I’m equally excited about is the prospect of a one-day treatment for latent TB. Together with the potential one-month treatment of active TB, we are calling this our “1 by 1” treatment strategy. Both treatment strategies combine the benefits of more potent, newer drugs coupled with improved drug delivery formulations, like long acting injectables.
New treatments alone can’t end TB; what else needs to happen to realize that vision?
Indeed, ultra-short, effective treatment for all forms of TB is necessary, but not sufficient to end TB. To accomplish that, as noted previously, we need further advances in both TB preventatives such as vaccines and TB diagnostics. However, above all, we need growing investment and political will in TB research and the provision of TB services. We need to propel parallel waves of innovation on the scale of the “1×1” in the worlds of diagnostics and vaccines, all of which require marked increases in investment.
Indeed, ultra-short, effective treatment for all forms of TB is necessary, but not sufficient to end TB. To accomplish that, as noted previously, we need further advances in both TB preventatives such as vaccines and TB diagnostics. However, above all, we need growing investment and political will in TB research and the provision of TB services. We need to propel parallel waves of innovation on the scale of the “1×1” in the worlds of diagnostics and vaccines, all of which require marked increases in investment.




We need to make TB a bigger tent. TB is not only the deadliest infectious disease in the world, but it’s so closely connected to additional issues like antimicrobial resistance, economic sovereignty, and even climate. We need to form global alliances committed to ending this ancient disease that has persisted for millennia. We need widespread personal investment that will then secure the necessary financial investment. We, frankly, need to do a much better job of generating the political will globally that will result in a commensurate investment in TB research and control, and allow us to realize a TB-free world.